Intelligent Multi-DOF Robotic Endoscope System with Sensorless Force Detection for Assistive Minimally Invasive Surgery
Main Project and Sub-project : Intelligent Multi-DOF Robotic Endoscope System with Sensorless Force Detection
 (1)Main Project: Intelligent Multi-DOF Robotic Endoscope System with Sensorless Force Detection for Assistive Minimally Invasive Surgery:
(1)Main Project: Intelligent Multi-DOF Robotic Endoscope System with Sensorless Force Detection for Assistive Minimally Invasive Surgery:
Laparoscopic surgery is a specialized technique for performing surgery. In traditional “open” surgery the surgeon uses a single incision to enter into the abdomen. Laparoscopic surgery uses several 0.5-1cm incisions. Specialized instruments and a special camera known as a laparoscope are passed through the trocars during the procedure. At the beginning of the procedure, the abdomen is inflated with carbon dioxide gas to provide a working and viewing space for the surgeon. The laparoscope transmits images from the abdominal cavity to high-resolution video monitors in the operating room. During the operation the surgeon watches detailed images of the abdomen on the monitor. This system allows the surgeon to perform the same operations as traditional surgery but with smaller incisions. Compared to traditional open surgery, patients often experience less pain, a shorter recovery, and less scarring with laparoscopic surgery.
(2)Sub-project 1: Intelligent Multi-DOF Robotic Endoscope System with Sensorless Force Detection:
Laparoscopic surgery is a specialized technique for performing surgery. In traditional “open” surgery the surgeon uses a single incision to enter into the abdomen. Laparoscopic surgery uses several 0.5-1cm incisions. Specialized instruments and a special camera known as a laparoscope are passed through the trocars during the procedure. Currently the CCD is operated by an assistant who is commanded by surgeon. The surgery time will become longer due to the bad teamwork between the assistant and surgeon. The proposal (Intelligent Multi-DOF Robotic Endoscope System with Sensorless Force Detection) provides a way to accord the different angle of the Motion Node which is mounted on the head of surgeon with an ENABLE/LOCK function to operate the position of the endoscope.
The system makes the surgeon can process the surgery and operate the endoscope himself simultaneously. To consider the safety issue, the proposal uses the impedance with velocity control, for the soft effect so the compliance control is used. The proposal Laparoscopic control will cover the D-H coordinate transformation and gravity compensation. Normally the traditional impedance control just consider the position and force control, the proposal provide an adaptive impedance control to implement the impedance with velocity control.
The force feedback will provide the moving resistance of the endoscope to surgeon. This design can avoid patient’s organ to be hurt by the moving endoscope. The system combines the advantages of the traditional laparoscopic surgery (TLS) and MIRS. Firstly, the system is intuitive operation without additional training. Secondly, because the system substitutes for endoscopic assistant, it can reduce manpower and improve surgical efficiency and efficacy. Thirdly, HMD with build in 3D visualization and force feedback assists surgeon with fully handling surgery.
(3)Sub-project 2: Medical Images Fusion and Respiratory Compensation in Laparoscopic Liver Surgery:
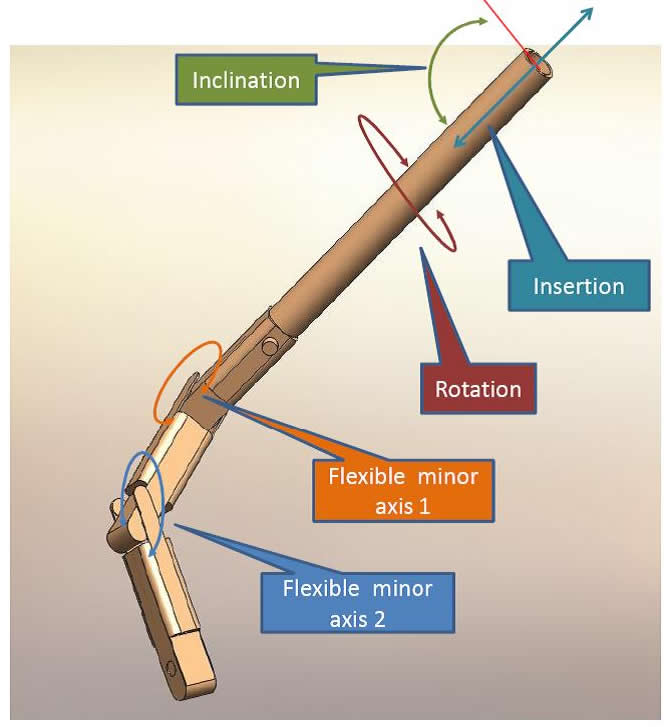
The purpose of this sub-project is to improve the front part of the laparoscope. The laparoscope that we have possesses the structure of the viewpoint adjustment and direction progression. And it is single/bi-session structure of rigid. The way of controlling is to adjust the axles of handler to adjust the direction.
There are 2 parts of improvement in our sub-project: The first one is to change the structure of rigid in to robustness in order to make the progression direction and viewpoint adjustment more flexible, make the space requirement much simpler and make it convenient to put into the supersonic probe. The second part is to revise the controlling method of back part into electronic-oriented mode. Thus the doctors can do the laparoscope adjustment through the method of designed human-machine interface.
We apply the developed laparoscope structure to implement the image-blended functional project. Besides putting the focal image that we acquired from the pre-surgery liver CT scan into human-machine interface and GPS system, we also utilize the immediate image that the supersonic reflected which is produced by the surgery procession, to conduct the correction of direction between soft tissue, laparoscopic image and pre-surgery image. And on the basis of this, we can overlap the focal into endoscopic image immediately. The doctors can fully get the information of focal via provided image-blending technique.
Finally, we embark on the improvement of human-machine interface, especially for the technique of image processing and image technique. We can effectively solve the problem of the movement of liver during the surgery through comparing the special biological character in the liver and image character. Thus we can compute and deduce the movement of liver. And we use the technique of image server to adjust the direction and the viewpoint immediately to make sure the image is located at visible region. Consequently, we can raise the safety and efficiency of the surgery.
(4)Sub-project 3: The applicability and reliability research of “Intelligent Multi-DOF Robotic Endoscope System with Sensorless Force Detection for Assistive Minimally Invasive Surgery”:
The laparoscopic surgery will be confirmed by the NTUH doctors to do the experiment on the live animals.